Demystifying the liver and it's diseases
 Demystifying the liver and it’s diseases
Demystifying the liver and it’s diseases
At a glance:
Functions of the liver include protein synthesis, detoxification, and metabolic processes.
Liver problems are often discovered incidentally through routine laboratory testing or screening blood tests.
Liver disease can have either an infectious or noninfectious etiology, such as hepatitis, nonalcoholic fatty liver disorders, and drug-induced injury.
Patients with nonalcoholic fatty liver disease or nonalcoholic steatohepatitis whose liver enzymes normalize after modificaiton of risk factors can be monitored conservatively and may avoid a liver biopsy.
Imaging is becoming more sensitive to fatty infiltration in the liver. Both ultrasonography and MRI can be useful.
The liver has a multitude of functions, including protein synthesis, detoxification, and metabolic processes. Problems in the liver are often discovered incidentally through routine lab testing or screening blood tests that include liver enzyme determinations. Abnormal results can make any practitioner nervous. Liver disease is like a puzzle: You need to put the pieces together to see the whole picture.
LIVER FUNCTION TESTS
A more descriptively accurate term for liver function tests (LFTs) might be “liver injury tests.” Some tests in the hepatic profile can tell you how well the liver is functioning. The most common determinations are those for bilirubin, aspartate aminotransferase (AST), alanine aminotransferase (ALT), total protein, albumin and alkaline phosphatase levels.
When an abnormal result is found, the clinician must figure out its origin. One of the most common reasons for referral to a hepatologist is elevated results on the LFTs. The tests most often found to have abnormal results include those for AST and ALT.
Hepatocyte injury.
For AST and ALT to become elevated, there must be injury to the hepatic tissues rich in these enzymes. The injury results in changes in cell permeability and leakage of AST and ALT into the blood. The more damage there is to the hepatocytes, the greater the leakage. ALT is more specific for liver injury than AST. Elevations in AST can also be the result of cardiac and muscle disease.
Cholestasis.
Patients with cholestasis will have elevations in their bilirubin, alkaline phosphatase (AP), and γ-glutamyltranspeptidase (GGT) levels. These elevations indicate damage to the bile ducts. AP is associated with the biliary tract but not specific to it. Elevations in AP can also be attributed to bone, placental and intestinal sources.
In the liver, AP is located in the hepatocyte membrane bordering the bile canaliculi. When this membrane is damaged, the enzyme is shed and AP levels in the blood become elevated. To help determine the etiology of an elevated AP level, the test can be fractionated into its various sources. This test will provide the concentration of AP attributable to each source as well as its percentage of the total. Depending on the laboratory, a normal AP level is usually <120 units/L.
GGT, like AP, is not specific to the liver. Alcohol intake can also cause elevations in the GGT. Sometimes the GGT can help differentiate the AP level with a hepatic etiology from other sources.
Bilirubin.
Bilirubin is a major breakdown product of hemoglobin and is derived from RBCs that have died and been removed by the spleen. During the degradation process, heme is separated out and the globin protein is transferred to the liver, where it is metabolized further in a process called conjugation.
Bilirubin that has gone to the liver and undergone further metabolic process is called conjugated bilirubin. This form of bilirubin is water-soluble and goes into the bile. The bilirubin that does not undergo this process is called unconjugated or indirect bilirubin.
On laboratory reports, the most commonly reported level is the total bilirubin. A patient who develops jaundice will typically have a total bilirubin level that is at least two to three times the upper limit of normal (normal level being <1.0 mg/dL). The total bilirubin level must be fractionated to further differentiate the causes of any abnormality.
Synthetic function.
The tests of synthetic function in the liver include prothrombin time (PT)/international normalized ratio (INR), platelet count and albumin level. Abnormal results indicate disease that has caused loss of proteins or inability to synthesize proteins. If a patient presents with hypoalbuminemia, thrombocytopenia (platelet count <150,000/µL)
and/or an elevated INR, the clinician should add advanced liver disease or cirrhosis to the list of differentials.
Other liver disorders.
The last two liver tests worthy of mention are miscellaneous assays of the ammonia and the α-fetoprotein (AFP) levels. An ammonia level is usually measured when a patient presents with acute changes in mental status because ammonia can cross the blood-brain barrier and become toxic to the brain. In liver disease, ammonia may build up because the liver cannot process it quickly enough or because an enzyme that breaks down the ammonia is absent or is present only in insufficient quantities. This can lead to hepatic encephalopathy in the patient with cirrhosis.
Ammonia levels, while useful, are primarily measured to rule out causes of changes in mental status. Ammonia levels are not always measured in hepatology practices. If the patient is mentating well, an elevated ammonia level may not mean anything. To use an old cliché, treat the patient, not the laboratory results.
AFP is a tumor marker for hepatocellular carcinoma (HCC) in patients with liver disease. The normal AFP level is <20 ng/mL. Most patients with hepatitis C have AFP levels that are <100 ng/mL. Any elevation in AFP warrants further investigation. Most concerning are elevated levels that continue to climb or levels found to be significantly elevated on first screening (i.e., in the several thousand range). The latest guidelines from the American Association for the Study of Liver Diseases do not recommend using AFP alone as a screening or diagnostic tool for HCC.1,2
Fibrosis markers.
Blood tests that can estimate the degree of fibrosis in the liver are relatively new. Each test, or marker, utilizes various methods to determine the stage of fibrosis. There are four stages of fibrosis in liver disease, so most test results will list four percentages. The F stage with the highest percentage is the one most likely in that particular patient. Fibrosis marker determinations are primarily beneficial for patients with minimal disease or advanced liver disease; the test is not as specific for the middle stages of fibrosis.
There are several fibrosis markers on the market, and each takes into account multiple factors when determining F scores. The advantage to fibrosis markers is that they are blood tests and not an invasive liver biopsy. Fibrosis markers can be useful in those for whom a liver biopsy is contraindicated or when the patient refuses the invasive procedure.
CLINICAL SCENARIOS
So now you have a patient with abnormal results on his or her liver function tests. Contrary to common belief, a basic workup can be done by any primary-care provider. Begin by determining if the abnormality is new or if the patient has a history of the problem.
Once the chronology of the event is determined, the abnormality can be further classified as hepatocellular, cholestatic or a combination of both. The most common issues are mild elevations of the aminotransferases (usually <100 IU/L). These tend to be hepatocellular in etiology. While significant elevations of the aminotransferases (>1,000 IU/L) can also be hepatocellular in origin, the differential diagnosis list in that instance is usually limited to such acute disorders as drug-induced liver disease, shock liver, fulminant hepatic failure, autoimmune hepatitis and acute hepatitis B.
In the patient with new-onset, mild AST/ALT elevations, the first step is to rule out alcohol ingestion and laboratory error, so rechecking the laboratory tests is indicated. How soon to repeat the tests depends on what the abnormality is. Most authorities recommend that testing be repeated anywhere from two to four weeks to three months later. If repeat testing reveals persistent AST/ALT elevations, i.e., >50 IU/L but <100 IU/L, the next step is to rule out diseases that cause hepatocellular injury. These can include both infectious and noninfectious disorders, such as hepatitis, nonalcoholic fatty liver disorders, and drug-induced injury.
Infectious hepatitis. One frequent cause of elevated AST/ALT is infectious hepatitis, most commonly hepatitis A, B, or C. (Other forms of infectious hepatitis are less common and will not be discussed in this article.) Acute infectious hepatitis can present with both elevated liver enzymes and vague symptoms, including anorexia and abdominal pain.
Hepatitis A is always acute in its presentation, whereas hepatitis B and C can have both acute and chronic presentations. Most acute hepatitis manifests with significantly elevated aminotransferases (>1,000 IU/L). For the patient who presents with acute elevations of AST/ALT, infectious hepatitis should always be in the initial differential.
Infectious hepatitis is easily ruled in or out with serologic testing, which must take into consideration the patient’s risk factors. The risk factors for hepatitis A, B, and C are presented in Table 1. Whether the patient has risk factors or not, these diseases should always be considered in such applicable populations as those with history of IV drug use (for hepatitis C virus HCV and hepatitis B virus HBV), men who have had sex with men (HBV), children born to a mother with HBV or HCV, and persons living in an area endemic for HBV.
Therapy for acute hepatitis comprises rest, nutrition, and fluids. A few cases of acute hepatitis will progress to acute liver failure. Prompt referral to a specialist is warranted for acute hepatitis that is not improving. Prevention of infectious hepatitis via vaccination is always recommended for appropriate individuals, such as health-care workers, people with liver disease or other chronic disease and those traveling to endemic areas.
Chronic hepatitis presents with mild AST/ALT elevations. According to the World Health Organization (WHO), approximately 350 million people live with chronic HBV infection3 and approximately 3% of the world’s population has been infected with HCV.4
Hepatitis B.
Patients who have chronic HBV infection may present with abnormal liver enzyme levels, fatigue, malaise, poor appetite and right upper-quadrant abdominal pain. Hepatitis B is diagnosed by serologic testing. The testing process is complex, and diagnosis relies on a number of assays, including those for hepatitis antigens (hepatitis B surface antigen HBsAg and hepatitis Be antigen HBeAg) and their respective antibodies (anti-HBsAg and anti-HBeAg), as well as antibodies to hepatitis B core antigen (anti-HBc immunoglobulin Ig M and IgG), and hepatitis B DNA.
The combination of results from all these assays will determine the diagnosis. For example, a patient who tests positive for HBsAg may have an acute or a chronic infection; results of the other assays will help to differentiate acute from chronic disease and determine the patient’s immune status. Table 2 provides a summary of possible results and their interpretation.
Most adults clear HBV before it progresses to chronic infection. However, for the patient who develops chronic disease, several medical therapies are available, including both oral and subcutaneous injection treatments, such as pegylated interferon alpha 2a (Pegasys), entecavir (Baraclude), adefovir (Hespera), telbivudine (Tyzeka), and tenofovir (Viread). Therapy should be started when the ALT elevation is more than two times the upper limit of normal, the patient has decompensated cirrhosis, or liver biopsy shows evidence of disease.5,6 Treatment of chronic hepatitis B requires the guidance of a specialist.
Hepatitis C.
The diagnosis of HCV infection is also based on serologic testing. Although several tests can be involved, the testing process is less complex than it is for HBV infection. Testing for HCV usually starts with an assay for the HCV antibody. This is only a screening test and is not diagnostic of HCV infection. The HCV recombinant strip immunoblot assay (RIBA) can help differentiate between exposure to HCV and actual infection.
Patients who test positive for HCV antibody need to be tested for virus in the serum. HCV RNA polymerase chain reaction (PCR) quantitative or HCV RNA qualitative testing is usually done next. Results of the qualitative test will be positive if any virus is detected in the blood, and the quantitative test will report the actual viral content. Some tests can detect a result as low as 43 IU/mL. A positive qualitative or quantitative test result is diagnostic for HCV infection. The actual viral count does not impact the severity of the disease. A patient with a viral load of
3 million copies/mL may not have more severe disease than the patient with a viral load of 1,000 copies/mL.
Therapy for chronic HCV infection is more complex than for other forms of hepatitis. Currently approved therapies include either daily doses of interferon alfacon-1 (Infergen) or weekly administration of pegylated interferon (Pegasys, Peg-interferon) with ribavirin (Copegus, Rebetol, RibaTab, Ribasphere). Two new adjunct therapies — the protease inhibitorstelaprevir (Incivek) and boceprevir (Victrelis) — were approved last year. These therapies are used in conjunction with pegylated interferon and ribavirin in treating HCV infection. They are currently approved for use in those with hepatitis C disease.
Telaprevir and boceprevir can be used in a person with cirrhosis, but the individual must have well-compensated disease as evidenced by a Child-Turcotte-Pugh classification score of “A.” The protease inhibitors are not currently approved for use in the post-transplant population. The new triple therapy had doubled the rates of sustained viral response (SVR). The SVRs of therapies range from 20% to 80%, depending on the degree of fibrosis and the genotype of the disease.
Patients with a confirmed diagnosis of HCV infection must be referred to a specialist for further evaluation. The specialist may choose to treat the patient or to perform liver biopsy. Because genotype 1 disease has the poorest rates of SVR, a liver biopsy is usually done to assess the extent of fibrosis.
Treatment is recommended in those with more advanced disease (stage 2+ fibrosis). Biopsy is not routinely done in patients with genotype 2 or 3 disease. Response to therapy is greatest in genotype 2 and 3 disease, and treatment is recommended in eligible patients regardless of disease severity.
Autoimmune hepatitis.
This form of hepatitis primarily affects women. The age at diagnosis varies. Autoimmune hepatitis has links to other autoimmune diseases, such as thyroiditis, Sjögren syndrome, and diabetes mellitus. At presentation, the patient may have either mild or significant elevations of the aminotransferases. Autoimmune hepatitis is also ruled out or in with laboratory testing. The serum test for autoimmune hepatitis is the antinuclear antibody test. A liver biopsy is often done to further diagnose the disease as well as to stage the extent of inflammation and fibrosis.
Treatment of autoimmune hepatitis usually consists of high-dose prednisone (started at around 40 mg/day) and possibly another immunosuppressant medication, such as azathioprine (Azasan, Imuran). The prednisone can be slowly tapered in some patients. Management of this disease requires the supervision of a specialist.
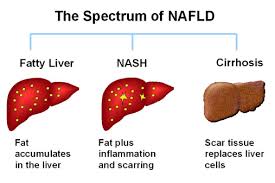
NAFLD and NASH.
Another common etiology of mild aminotransferase elevations is nonalcoholic fatty liver disease (NAFLD) or a more progressive form of obesity-related liver disease called nonalcoholic steatohepatitis (NASH). NAFLD is an equal-opportunity disease, affecting 20% of adults and 5% of children.7
NASH results from fat deposition in the liver (steatosis). Possible sequelae to this disorder include cirrhosis and HCC.2 We are still learning why patients progress from NAFLD to NASH. Elevations in fatty acids/triglycerides, obesity, and insulin resistance have all been associated with NASH. (See Table 3 for a more extensive list of associated conditions.) While some data have linked elevated triglycerides with NASH, the problem likely occurs when fatty acids accumulate because the fatty acid supply overwhelms triglyceride synthesis.2
NAFLD and NASH will likely not progress within the first few months of diagnosis. Many clinicians will monitor a patient after initial workup and make medical recommendations to lose weight or control diabetes mellitus (if applicable). Patients whose liver enzymes normalize after modifying their risk factors can be monitored conservatively and may avoid a liver biopsy. If the aminotransferase elevations persist, however, the patient requires referral to a specialist for a liver biopsy and further evaluation.
Ultrasonography and MRI have become more sensitive to fatty infiltration in the liver. The gold standard in diagnosing NAFLD and NASH is a liver biopsy. Liver biopsy carries risk factors and should be ordered only after other workup has been completed. Figure 1 is an algorithm for the evaluation of patients suspected of having NAFLD.
CONCLUSION
Just as the liver has numerous functions, so does it have the potential for dysfunction. Primary-care clinicians with an understanding of basic liver function can begin the diagnostic process, recognizing that patients with more serious liver disorders may require the supervision of a hepatologist.